







Evaluation of PulmonaryNodules
Adam Guttentag M.D.
All photos retain the copyrights of their original authors
© Adam Guttentag, MD
Solitary Pulmonary Nodule
Focal mass lessthan 3 cm indiameter

Solitary Pulmonary Nodule
Long differential diagnosis.
About half of nodules seen on CXR will beneoplasm.
Primary lung cancer
Carcinoid
Metastasis
Malignant rate of those seen by CT issmaller due to their smaller size.
Pulmonary Nodule
First…you must see it.
Missed Nodules
Failure of search
nodule never scanned by viewer’s eye
“Tunnel vision” (looking for something else)
Satisfaction of search (“instant happiness” syndrome)
Failure of perception
area of nodule scanned but no nodule is recognized
most common cause of a true miss
failure to compare with old films
Errors of interpretation
nodule noted but interpreted as something else

Common locations ofmissed nodules
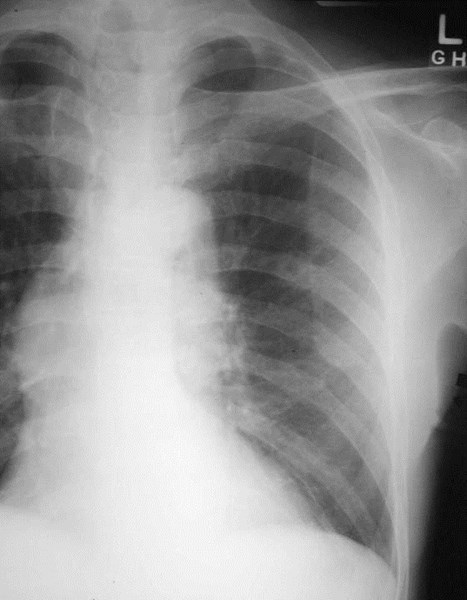
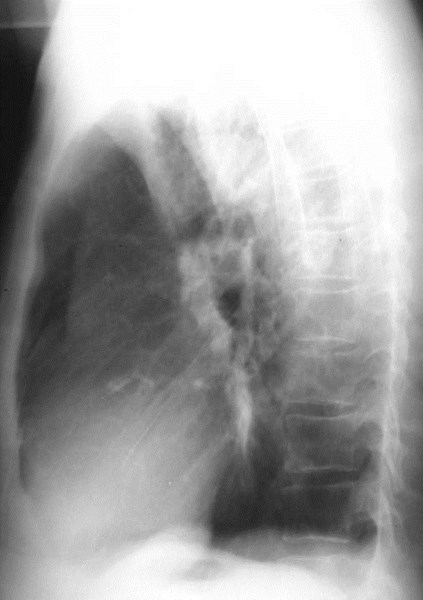
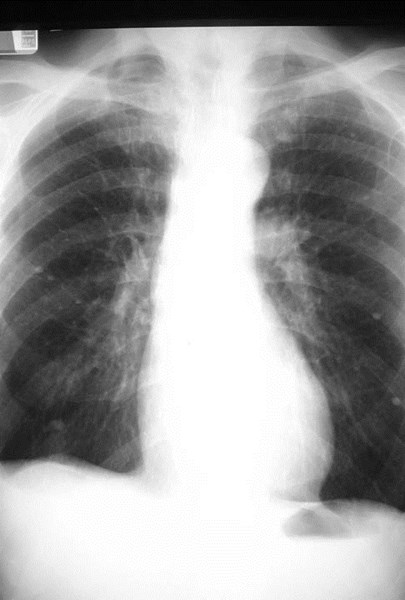
Quick– do you see a nodule?
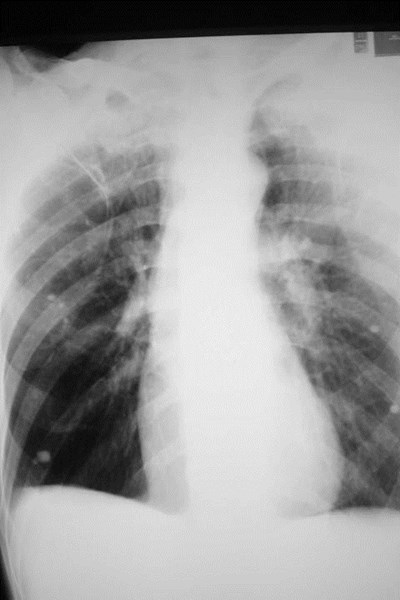
How about now?
Low density nodule ishard to see if hidingunder a rib


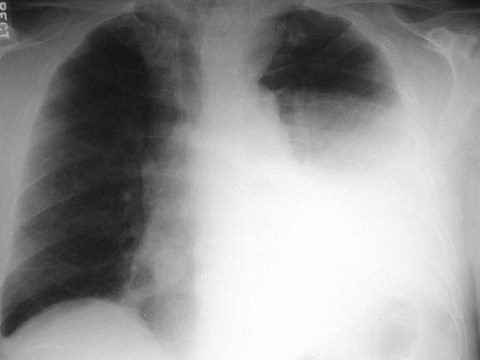
Beware of tunnel vision!
Critical Questions
Is it new or growing?
GET OLD FILMS!
Even if it’s from another facility.
Stability for more than two years implies benignity.
Avoid the entire worry and workup!
Is it in the lung?
Beware of calcified rib ends, skin tags, pleural plaques, boneislands, nipples, etc.!
What does it look like?
Techniques for NoduleEvaluation
Start simple if you can!
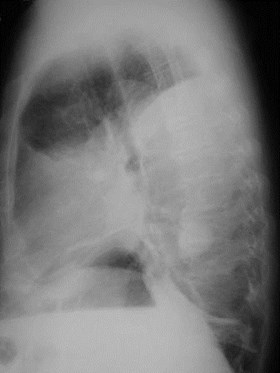
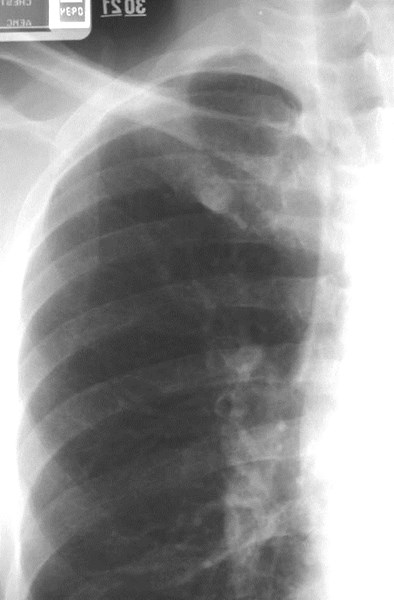
Oblique or lordotic views
Low kVp films (rib technique)
CT
(MRI)
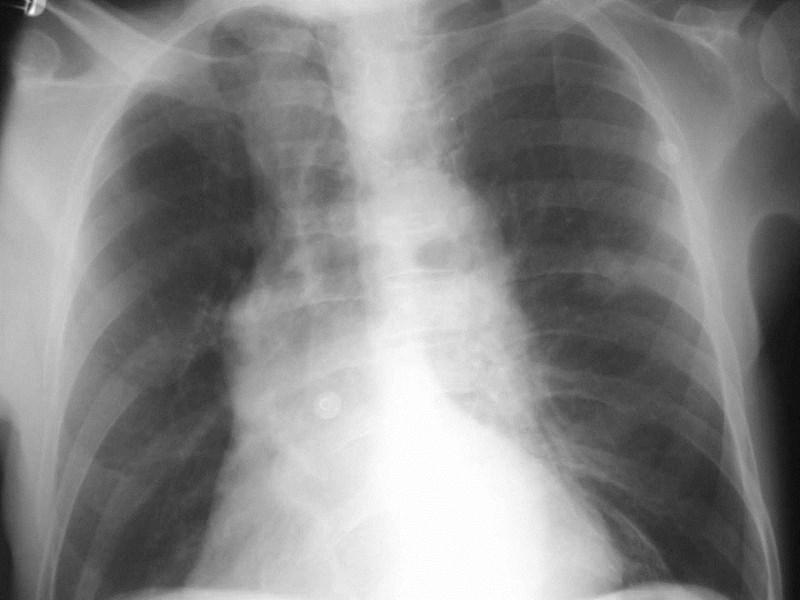
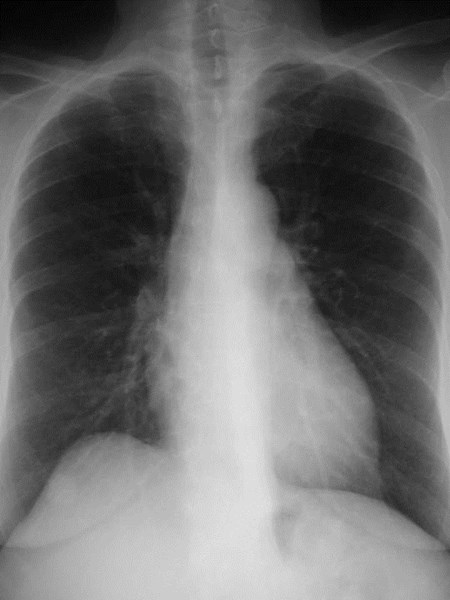
Nipple shadows


?
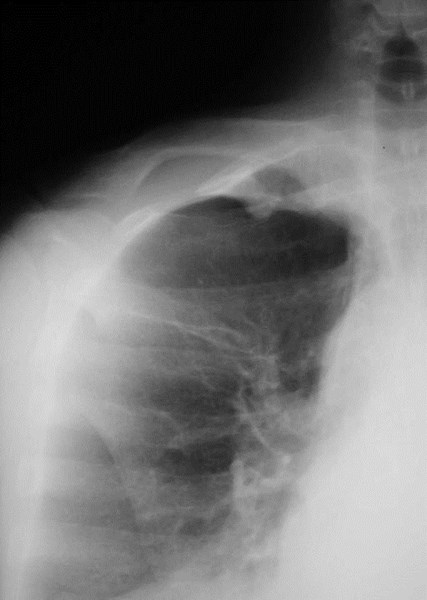
Apical lordotic view
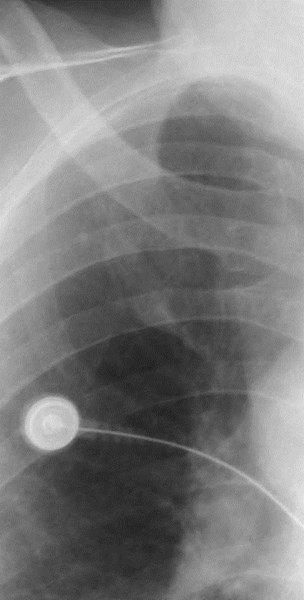

Old film
Standard technique
Rib technique
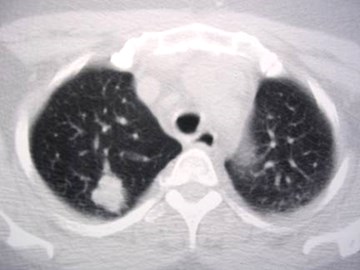
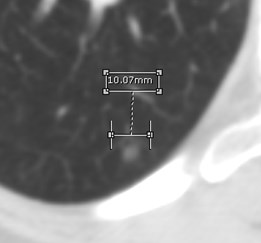
CT — what to evaluate
Size
Borders
Internal characteristics
Enhancement
Location/bronchial relations
Needle vs. bronchoscopic bx
ARE THERE ANY OTHER NODULES?
Changes differential diagnosis
Does Size Matter?
Masses >3 cm : >80% are malignant.
Nodules <2cm: 80% are benign.
But: 42% of cancers are <2 cm and 15%are <1 cm
These will increase as more cancers are foundincidentally or by screening
Borders
Malignant
Lobulated
Spiculated
Irregular
Borders
Benign
Smooth
(but 21% of malignantnodules are smooth,esp. metastases)

Calcification
Benign
Only 38-63% ofbenign nodules
Laminated
Dense central(“popcorn”)
Entire nodule
Malignant
Ca++ seen in up to 6% ofcases
Stippled
Granular
Eccentric
Especially common incarcinoid tumor, adenoCa

Hamartoma:“Popcorn”Ca++


Granuloma:laminatedCa++


Squamous cellCa: “stippled”Ca++
Patterns ofcalcification
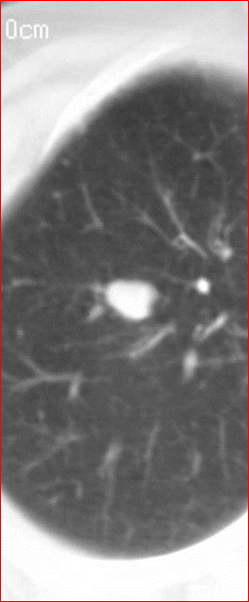
Other benign characteristics
Fat in nodule
Density -40 HU to -120 HU
Seen in 50% of hamartomas
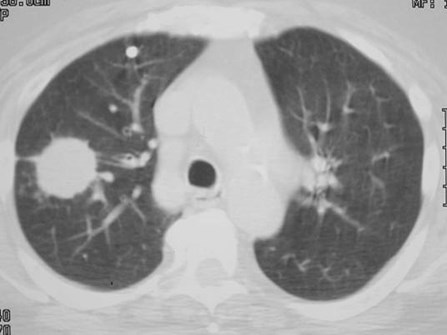
Smooth cavity wall, <4mm thick
Wall >16mm is usually malignant

Hamartoma with fat
The Indeterminate Nodule
Unfortunately, this includes most nodules.
No benign features:
Fat
Benign calcification
Stability of size
Sometimes it’s easy…
Evaluation of indeterminatenodules
Growth rate
Need old study to compare
Doubling time <30 or >730 days almostalways means benign
REMEMBER: doubling in volume means only a4 → 5 mm diameter growth.
So very subtle growth in diameter can mean adoubling in volume
Tiny nodules are hard to measure consistently
Need thin sections for measurement
Evaluation of indeterminatenodules
Risk assessment using Bayesian analysis
Uses nodule and patient characteristics
E.g.: age, smoker, size, location,growth rate
Determine probability of malignancy (Pca)using likelihood ratios (LR)
Likelihood ratios for individualcharacteristics
Spiculated margin5.54
>3 cm5.23
>70 y.o. 4.16
Malignant growth rate3.40
Smoker2.27
Upper lobe1.22
<1 cm0.52
Smooth margins0.30
30-39 y.o. 0.24
Never smoked0.19
20-29 y.o. 0.05
Benign calcification0.01
Benign growth rate0.01
Bayesian analysis
Example: smooth 8 mm SPN
35 y.o. nonsmoker Pca = 0.01
70 y.o. smoker Pca = 0.50
Observe 1st patient, biopsy 2nd
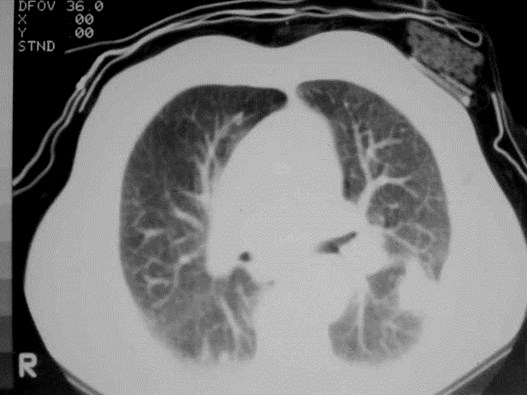
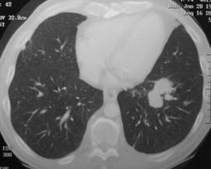
CT nodule enhancement
“Poor man’s PET”
CT enhancement
Give bolus of IV contrast, scan repeatedlythrough nodule over ~5 minutes
Need good technique, thin slices, nomotion or other artifact
Need nodule at least 6-8 mm
CT nodule enhancement
Increase in nodule density more than 15 HU:
High sensitivity for dx of cancer (98%)
Few false negatives
Fair specificity (58%)
Some benign lesions enhance.
Raising threshold to 20 HU increases specificity
Very good as negative test.


19 HU
54 HU
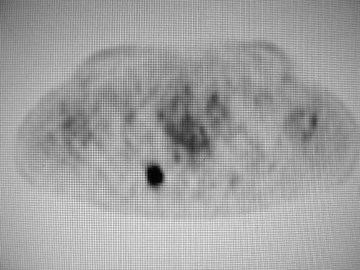
Positron Emission Tomography(PET)
Uptake of FDG is related to glucosemetabolism of tissue
Low uptake usually = benign
Very few malignant nodules >1 cm arecalled benign
High sensitivity for malignancy
Some benign nodules have uptake
Lower specificity for malignancy
(See CT enhancement)
PET
For benign nodules:
Sensitivity = 96%
Specificity = 88%
Accuracy = 94%
Negative result in SPN >1 cm allowsradiographic follow up.
False negatives: Well differentiated cancer(BAC) and carcinoid.
PET


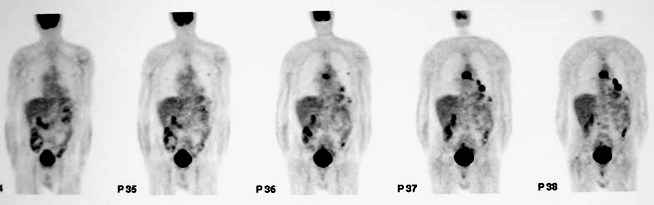
Primary tumor
Mediastinal nodes
Pulmonary mets
PET
Beware the false positive!
Granulomatous diseases and chronic inflammation
Needle biopsy = TB
The Real Problem
You’ve found a nodule!
Now… you must decide what the heck todo about it.
What to do with your patientwith a nodule?
Is it likely to be cancer?
How big is it?
Nodule >1 cm: plenty of options:
CT follow up
PET
CT enhancement
FNABx
Nodule <1 cm
Difficult to biopsy with needle
PET not reliable as negative test
CT enhancement difficult because of volume averaging, motion
Bronchoscopy has poor sensitivity
Small pulmonary nodules
High prevalence of indeterminatepulmonary nodules in asymptomatic highrisk patients at CT:
Mayo Clinic (MN): 51%
89% <8mm
22 cancers in 1500 patients screened (1.5%)
ELCAP study (NYC): 23%
27 cancers in 1000 patients screened (2.7%)
Ditzels
We see lots of tiny nodules (“ditzels”) <5mm
More and more as scanners get better and slicewidth gets thinner.
We don’t really know what to do with them.
Tiny nodules are overwhelmingly benign.
But…all cancers start small, don’t they?
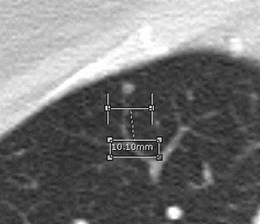
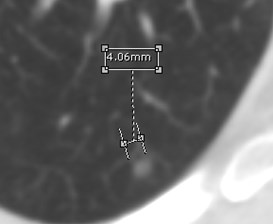
Follow up of nodules — how soon?
Say a nodule grows from 4 to 5 mm.
It has doubled in volume.
But is that real? It’s hard to measure nodules that small.
Measurement depends on measurer, phase ofinspiration during scan, windowing of image.
Accurate measurements are critical to follow up.
Early CT follow up:Wasting time?
Average doubling time for smallsolid nodules is about fivemonths.
It’s unlikely that a tiny nodulewill grow more than 1 mm in 3months
If we can’t be sure that a nodulehas grown, it makes no sense tofollow these tiny nodules in 3months.
Ditzels
For nodules <10 mm: does early (< 12 month)follow up allow earlier cancer dx?
Retrospective look at ELCAP (NYC screening) data:
For 378 nodules <5mm, none would have beendiagnosed as cancer based on early repeat CT.
Uncertain or no growth seen on early repeat CT, or noneat 12 month follow up.
For 238 nodules 5-9mm, 13 (5%) would have beendiagnosed as cancer based on early repeat CT.
Argument for earlier follow up of nodules >5mm.
Henschke et al Radiology 2004;231:164-168Henschke et al Radiology 2004;231:164-168
Does it cause harm to follow upnodules that prove malignant?
For cancers <3 cm, there is controversy aboutwhether survival is better with smaller tumorsize.
Highly malignant tumors are likely metastasize whilestill small. Survival for stage 1A tumors only 50-85%
For less aggressive tumors, staging will not change ifbiopsy or surgery is delayed for several months.
So there may be no harm in waiting to be sure asmall nodule is growing before pursuingaggressive dx.
Risk of delayed diagnosis must be balanced byrisks and expense of invasive diagnostic tests ormultiple follow up CT scans.
Fleischner Societyproposed follow up recommendationsfor small solid nodules
Low risk patients
<4mm, no F/U
4-6 mm, F/U in 12 months,stop if no change.
6-8mm, F/U in 6-12 months,then up to 18-24 months if nochange.
>8mm, CT F/U 3, 9, 24 monthsor PET/enhanced CT/bx
High risk patient
<4mm F/U 12 months, stop ifno change
4-6 mm, F/U 6-12 months, then18-24 months if no change
6-8 mm, F/U 3-6 months, then18-24 months if no change
>8 mm, same as for low riskpatients
Review Questions
For a patient whose chest radiograph shows a10mm pulmonary nodule, the appropriate nextstep is:
1.PET scan
2.CT scan
3.Oblique radiographs with nipple markers
4.Search for old chest radiograph
Appropriate diagnostic tests for a new 15mm nodule in a smoker include all except:
1.CT scan
2.PET scan
3.Needle biopsy
4.MRI scan
Appropriate follow up for a 3 mm nodulediscovered incidentally in a 45 year oldsmoker:
1.None
2.6-12 month CT scan without contrast
3.PET scan
4.Wedge resection
5.Pulmonary consultation
Additional reading
Swenson et al: Lung nodule enhancement at CT:multicenter study. Radiology 2000; 214: 73-80.
Henschke et al CT screening for lung cancer:suspiciousness of nodules according to size on baselinescans. Radiology 2004; 231:164-8.
Gupta et al: Mediastinal lymph node sampling followingFDG-PET imaging in lung cancer staging.Chest 2001;120:521-7.
Cummings SR et al Estimating the probability ofmalignancy in solitary pulmonary nodules. A Bayesianapproach. Am Rev Respir Dis 1986 134(3):449-52.
The End
Use the back button on the browser to exit the program